National Blood Authority
AUSTRALIAN HAEMOVIGILANCE REPORT
A report by the National Blood Authority Haemovigilance Advisory Committee
The transfusion of blood and blood components is a core part of healthcare service delivery to patients. While the use of blood and blood components can be lifesaving, there are also risks associated with their transfusion. In Australia, the risk of transmission of infectious disease (such as HIV, hepatitis B and C) through blood transfusions has reduced significantly in recent years through improved manufacturing and laboratory processes. However, in common with other developed countries, the non-infectious risks of transfusion, especially those related to human errors, continue to occur and affect patients' safety and health.
The mechanisms to ensure the safety of transfusions in Australia include:
Surveillance of adverse transfusion events is the cornerstone of haemovigilance systems. However, there are many ways in which haemovigilance is defined. A founding definition of haemovigilance was set out in Directive 2002/98/EC of the European Parliament[1], setting standards of quality and safety for the collection, testing, processing, storage and distribution of human blood and blood components:
'A set of organised surveillance procedures relating to serious adverse or unexpected events or reactions in donors or recipients, and the epidemiological follow-up of donors'
The International Haemovigilance Network(IHN)[2] definition is the one most widely used and it states:
'A set of surveillance procedures covering the whole transfusion chain (from the collection of blood and its components to the followup of recipients), intended to collect and assess information on unexpected or undesirable effects resulting from the therapeutic use of labile blood products, and to prevent their occurrence or reccurrence.[3]'
Haemovigilance is now universally recognised as an integral part of safety in blood transfusion, and increasing attention is being paid to haemovigilance in many countries. The World Health Organization (WHO) Global Database on Blood Safety Summary Report 2011[4] indicates that a national haemovigilance system was present in 13% of low-income countries, 30% of middle income countries and 78% of high-income countries (data based on 106 responding countries). National haemovigilance systems provide an evidence base for the improvement of transfusion practice that displays the real risks and hazards of transfusion in a given community/country and allows for the dissemination of these findings and the instigation of appropriate actions, including educational processes to prevent reccurrence.
All developed countries are facing increased demand for blood and blood products. Ageing populations and decreased donations contribute to competing supply and demand pressures for blood resources.[5]
In Australia, blood is voluntarily donated free from financial incentive. The Blood Service collects and processes blood and distributes blood products to Australian health providers in accordance with government policies in the National Blood Agreement and National Blood Authority Act 2003.
The NBA coordinates the purchase and supply of blood and blood products on behalf of all Australian governments. The Blood Service is funded by all Australian governments through the NBA which contracts the Blood Service under a Deed of Agreement. The Therapeutic Goods Administration (TGA) regulates blood and plasma manufacturing activities and monitors any serious adverse transfusion events that may be product related.
|
2009-10 |
RBC |
Platelets |
FFP |
Cryoprecipitate |
Cryodepleted plasma |
|
Units |
Units |
Units |
Units |
Units |
|
|
NSW |
247,432 |
35,192 |
57,923 |
25,333 |
2,351 |
|
VIC |
207,004 |
33,043 |
32,887 |
17,432 |
1,675 |
|
QLD |
169,139 |
35,958 |
38,405 |
9,074 |
5,446 |
|
WA |
68,044 |
8,915 |
12,722 |
5,809 |
1,129 |
|
SA |
71,226 |
9,661 |
14,566 |
1,539 |
633 |
|
TAS |
15,235 |
2,792 |
1,503 |
1,472 |
0 |
|
ACT |
12,535 |
2,066 |
2,234 |
1,409 |
133 |
|
NT |
5,278 |
868 |
574 |
281 |
0 |
|
Australia |
795,892 |
128,495 |
160,814 |
62,349 |
11,367 |
|
2010-11 |
|||||
|
Units |
Units |
Units |
Units |
Units |
|
|
NSW |
252,792 |
38,191 |
57,384 |
28,472 |
5,729 |
|
VIC |
207,828 |
33,959 |
35,182 |
18,524 |
2,699 |
|
QLD |
167,051 |
37,167 |
39,418 |
9,428 |
3,430 |
|
WA |
66,012 |
9,139 |
10,771 |
6,436 |
669 |
|
SA |
71,782 |
10,168 |
12,522 |
3,402 |
390 |
|
TAS |
15,715 |
3,267 |
1,748 |
1,891 |
48 |
|
ACT |
13,346 |
1,804 |
2,487 |
1,677 |
322 |
|
NT |
6,047 |
1,010 |
1,026 |
258 |
595 |
|
Australia |
800,571 |
134,704 |
160,538 |
70,088 |
13,882 |
Source: NBA
Notes
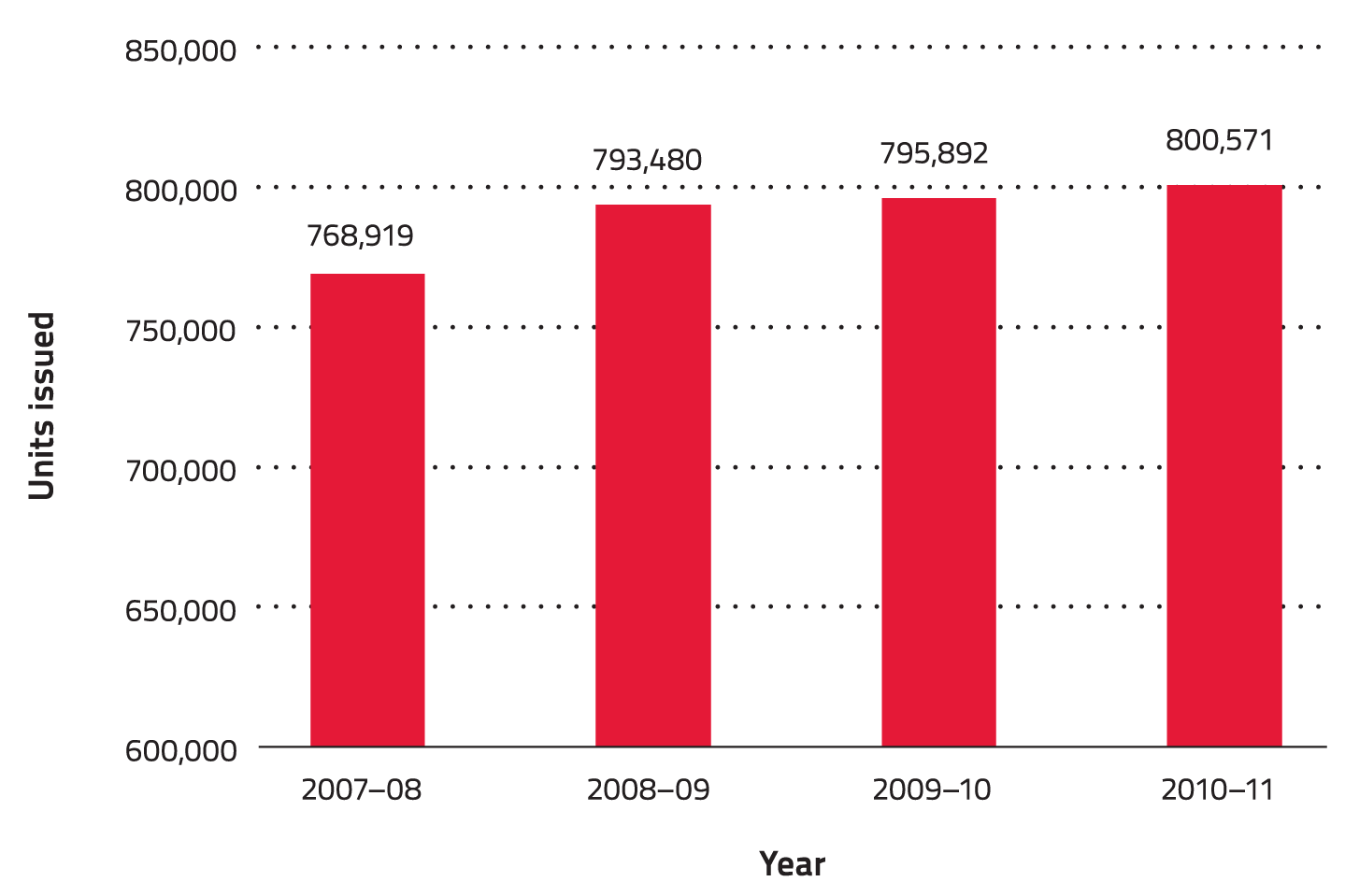
From 2009-10 to 2010-11, there were about 2.3 million components of fresh blood products issued in Australia. The demand for red blood cells remained high, accounting for about two-thirds of all issues. The demand for blood components varied across states and territories. NSW accounted for about 32% of all issues, followed by VIC (25%) and QLD (22%). NT accounted for less than 1% of all issues.
In line with many developed countries Australia has made increasing progress towards improving the efficiency of blood utilisation and clinical transfusion practice. Transfusion-related clinical practice improvement programs in a number of states and territories have continued to develop in areas such as appropriate use of blood, clinical governance, haemovigilance and ongoing education of clinical and associated health care professionals.
The following tables (Table 2, Table 3) and figures (Figure 1, Figure 2) show that:
|
Blood component |
2007-08 |
2008-09 |
2009-10 |
2010-11 |
|
RBC units |
768,919 |
793,480 |
795,892 |
800,571 |
|
Platelets (adult equivalent doses) |
116,665 |
118,248 |
128,495 |
134,704 |
|
Fresh frozen plasma units |
144,987 |
152,689 |
160,814 |
160,538 |
|
Cryoprecipitate units |
53,459 |
59,267 |
64,734 |
70,102 |
|
Cryodepleted plasma units |
14,888 |
15,430 |
11,872 |
13,882 |
Source: NBA
Note: RBC=Red blood cell
|
Blood component |
2007-08 |
2008-09 |
2009-10 |
2010-11 |
|
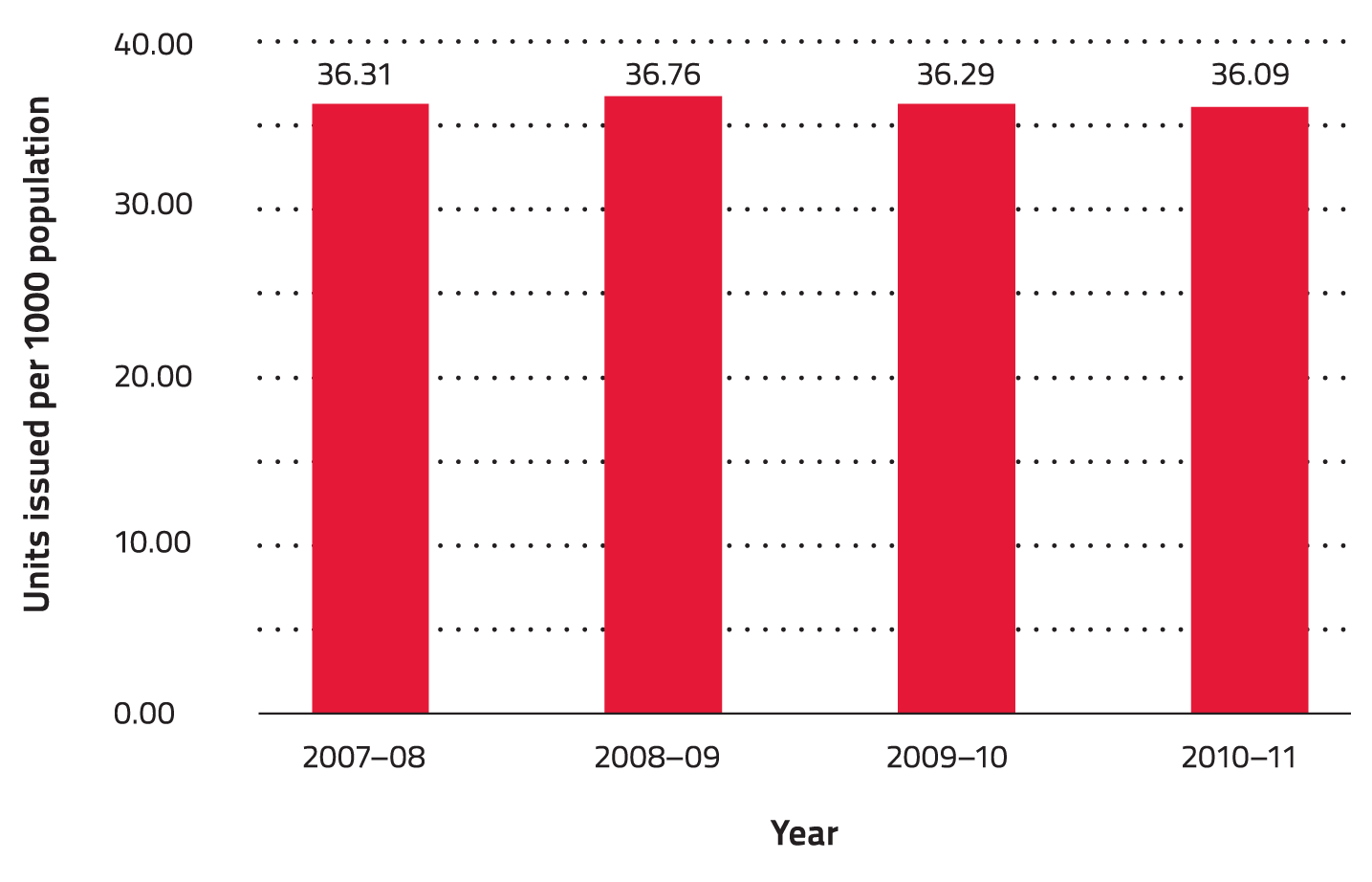
RBC units |
36.31 |
36.76 |
36.29 |
36.09 |
|
Platelets (adult equivalent doses) |
4.80 |
5.48 |
5.86 |
6.07 |
|
Fresh frozen plasma units |
6.85 |
7.07 |
7.33 |
7.24 |
|
Cryoprecipitate |
2.52 |
2.75 |
2.95 |
3.16 |
|
Cryodepleted plasma units |
0.70 |
0.71 |
0.54 |
0.63 |
Source: NBA
Notes
Figure 1: Total red blood cell issues in Australia, 2007-08 to 2010-11
Source: NBA
Figure 2: Total red blood cell issues per 1000 population, 2007-08 to 2010-11
Source: NBA
Australia's population continues to rise at a slow pace increasing by 1.4% during the year ended 30 June 2011. The growth rate has been declining since the peak of 2.2% for the calendar year ended 31 December 2008.[7] Increases in population will inevitably result in increased future demand for health care services, including blood and blood components.
Australia's population, similar to that of most developed countries, is ageing as a result of sustained low birth rates and increasing life expectancy. This is resulting in proportionally fewer children (less than 15 years of age) in the population. The median age (the age at which half the population is older and half is younger) of the Australian population increased by 4.7 years over the last two decades, from 32.4 years at 30 June 1991 to 37.1 years at 30 June 2011. Between 30 June 2010 and 2011 the median age rose slightly from 36.9 to 37.1. Over the next several decades, population ageing is projected to have significant implications for Australia including increased demands on the health system.[8]
Australia enjoys one of the highest life expectancies in the world. In 2009 it was ranked fifth overall at 81.6 among Organisation for Economic Co-operation and Development (OECD) countries after Japan (83.0 years), Switzerland (82.3), Italy (82.0) and Spain (81.8).[9]
In the 12 months to 30 June 2010, the number of people aged 65 years and over in Australia increased by 97,600 people, representing a 2.4% increase. The proportion of the population aged 65 years and over increased from 11.3% to 13.7% between 30 June 1991 and 30 June 2011. In the 12 months to 30 June 2011, the number of people aged 85 years and over increased by 20,900 people (5.3%) to reach 415,400. Over the two decades to 30 June 2011, the number of people aged 85 years and over increased by 169% compared with a total population growth of 31% for the same period.[6]
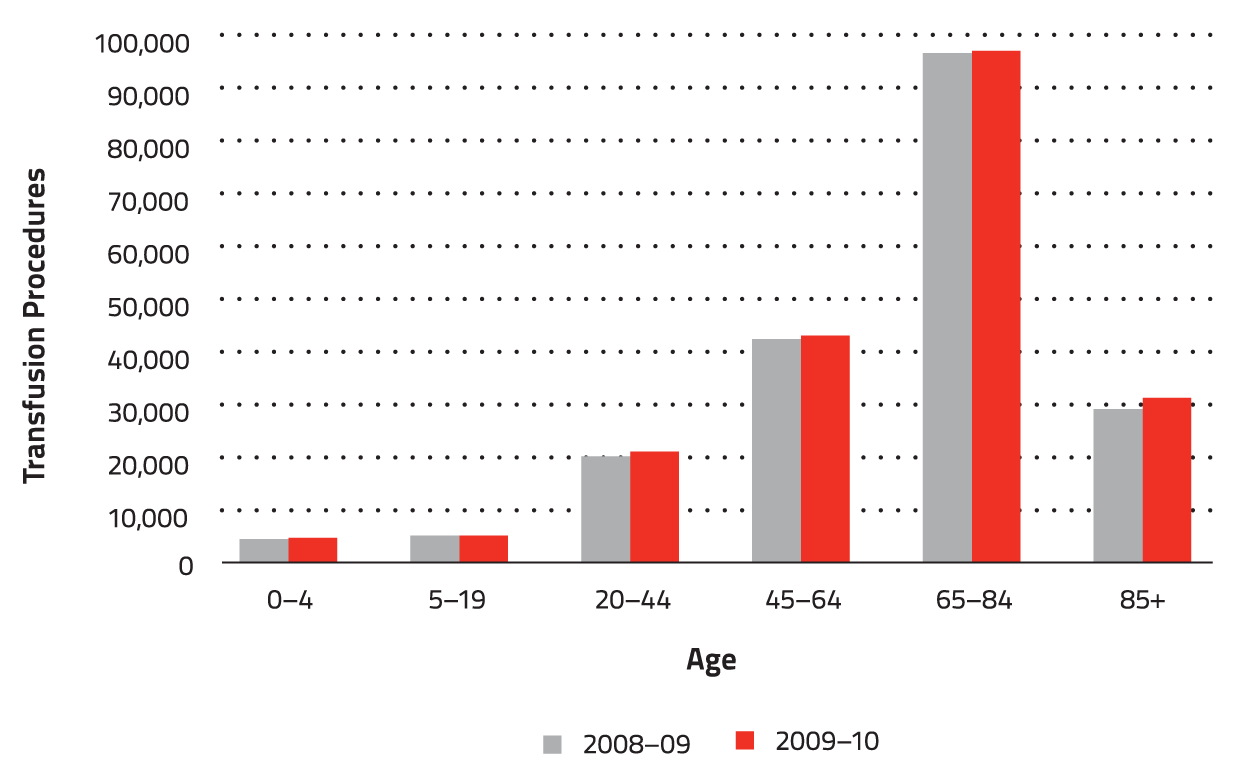
The rise in the elderly population of Australia has a tangible effect on the nation's blood supply needs. There is a correlation between patient age and blood component use and this is illustrated by a range of data available from the Australian Institute of Health and Welfare (AIHW).
The AIHW publishes data relating to transfusion of blood and immunoglobulin on an annual basis. There are, however, a number of limitations[10] with respect to the analysis and the potential use of this data for blood supply demand planning:
Despite the limitations, the AIHW data provides some insight into Australian transfusion trends.
Figure 3 shows that the majority of red cell transfusion procedures in 2008-09 and 2009-10 occurred in patients aged 65 years and over. A similar trend was also observed for the other blood components (Table 4, Table 5) for the same period.
This phenomenon is not unique to Australia. Epidemiological information from the United States, England, and Denmark highlighted similar age and sex distributions of transfused patients:[11]
Figure 3: Red cell transfusions by patient age, 2008-09 and 2009-10
Source: AIHW National Hospital Morbidity Database
|
|
Number of Procedures |
Percentage of Procedures |
||||||||||
|
Transfusion of |
0-4yrs |
5-19yrs |
20-44yrs |
45-64yrs |
65-84yrs |
85+ |
0-4yrs |
5-19yrs |
20-44yrs |
45-64yrs |
65-84yrs |
85+ |
|
Whole blood |
76 |
276 |
1,937 |
548 |
456 |
150 |
2% |
8% |
56% |
16% |
13% |
4% |
|
Red blood cells |
4,430 |
5,030 |
20,070 |
42,276 |
96,516 |
29,092 |
2% |
3% |
10% |
21% |
49% |
15% |
|
Platelets |
1,708 |
1,786 |
3,450 |
9,242 |
11,618 |
1,091 |
6% |
6% |
12% |
32% |
40% |
4% |
|
Leukocytes |
1 |
2 |
4 |
40 |
10 |
2 |
2% |
3% |
7% |
68% |
17% |
3% |
|
Autologous blood |
145 |
207 |
419 |
3,084 |
4,338 |
290 |
2% |
2% |
5% |
36% |
51% |
3% |
|
Other serum |
1,825 |
1,123 |
4,899 |
12,677 |
17,857 |
2,912 |
4% |
3% |
12% |
31% |
43% |
7% |
|
Blood expander |
22 |
73 |
838 |
2,028 |
3,329 |
516 |
0% |
1% |
12% |
30% |
49% |
8% |
|
Other substance |
1,378 |
4,034 |
10,328 |
20,480 |
18,635 |
1,535 |
2% |
7% |
18% |
36% |
33% |
3% |
Source: AIHW National Hospital Morbidity Database
Notes
|
|
Number of Procedures |
Percentage of Procedures |
||||||||||
|
Transfusion of |
0-4yrs |
5-19yrs |
20-44yrs |
45-64yrs |
65-84yrs |
85+ |
0-4yrs |
5-19yrs |
20-44yrs |
45-64yrs |
65-84yrs |
85+ |
|
Whole blood |
121 |
291 |
1,944 |
502 |
306 |
136 |
4% |
9% |
59% |
15% |
9% |
4% |
|
Red blood cells |
4,609 |
5,137 |
20,981 |
43,018 |
97,041 |
31,311 |
2% |
3% |
10% |
21% |
48% |
15% |
|
Platelets |
1,785 |
1,966 |
3,820 |
9,789 |
13,166 |
1,425 |
6% |
6% |
12% |
31% |
41% |
4% |
|
Leukocytes |
15 |
7 |
21 |
26 |
24 |
3 |
16% |
7% |
22% |
27% |
25% |
3% |
|
Autologous blood |
126 |
197 |
482 |
3,363 |
4,760 |
308 |
1% |
2% |
5% |
36% |
52% |
3% |
|
Other serum |
2,056 |
1,260 |
5,543 |
14,160 |
19,446 |
3,186 |
5% |
3% |
12% |
31% |
43% |
7% |
|
Blood expander |
9 |
46 |
670 |
1,771 |
2,645 |
460 |
0% |
1% |
12% |
32% |
47% |
8% |
|
Other substance |
1,629 |
4,186 |
11,103 |
22,191 |
21,694 |
1,756 |
3% |
7% |
18% |
35% |
35% |
3% |
Source: AIHW National Hospital Morbidity Database
A number of international studies have been undertaken examining changes in red cell usage over time, with particular focus on the impact of an ageing population.[12],[13],[14] As elderly patients are the main users of blood components, concerns have been raised that an ageing population may result in an increased demand for blood components.
The above studies show, despite an ageing population, the RBC demand may not increase as much as predicted by other studies and further deceases in surgical RBC use may be achievable. However, a total increase in population numbers where that population is also ageing is likely to demand more blood for medical use. As a substantial user of RBCs and blood products, clinical haematology should be a target for best practice initiatives.
These results are consistent with similar studies undertaken by groups in other developed countries with similar ageing population profiles. The Blood Service 'Bloodhound' study[18] showed a similar age profile for Australian patients receiving red cell transfusions, with the median age of recipients being 69 years. The Bloodhound study following the fate of 5,052 RBC units indicated that for 53.4% of blood units the urgency of the surgical procedure and the urgency of transfusion was less than 24 hours. Only a small proportion was shown to support elective surgery.
Approximately one-third of tagged red blood cells were used to support surgery, one-third for haematology/oncology and one-third for other medical and miscellaneous indications. The breakdown of the clinical indications for transfusion was as follows:[18]
Epidemiological information from the United States, England, Australia and Denmark suggests that the relationship between the disease or surgical procedure and the use of blood components was similar between these developed countries.[11] The use of red blood cells in cardiovascular surgery predominated. Neoplasms and digestive disorders were also common. Neoplasms, including those relating to haematology, were the main cause of platelet use, but cardiovascular surgery was also important. In all countries, plasma was largely used in cardiovascular surgery. Two countries provided data relating to the number of units per transfusion episode including information relating to massive transfusion. In Australia, red cell use of ≥50 units per episode was largely associated with multi-trauma patients.
Haemovigilance is a vital and integral part of modern transfusion medicine. In Australia, national haemovigilance reporting is voluntary (with the exception of sentinel events, see APPENDIX II: DEFINITIONS IN HAEMOVIGILANCE) but is seen as part of the professional duty of care for patient safety. Health service organisations have been recommended by the national government to participate in relevant haemovigilance activities conducted either locally or at state or national level from 1 January 2013. Haemovigilance provides a very important source for identifying emerging trends in hazards related to blood transfusion. The quality of blood and blood products in Australia has reduced the recorded risks associated with the transfusion product itself that are captured in many other haemovigilance systems around the world. The major residual hazards of transfusion in Australia can be broadly divided into human errors and clinical reactions.
In common with other OECD countries, such as the United Kingdom, New Zealand, Sweden and Canada, the risks to the safety of transfused patients in Australia have clearly been shown to occur predominantly in the hospital environment arising from human errors. For example, the majority of preventable transfusion errors and adverse events result from human error.
In order to help national haemovigilance programs to collect comparable international data, the International Society for Blood Transfusion (ISBT) has developed standard definitions for non-infectious adverse transfusion reactions.[19] The HAC has adopted these definitions and included them in the Australian National Haemovigilance Data Dictionary for national reporting.
The objectives of a national haemovigilance system are to provide an evidence base for improvement of transfusion practice, to know what the real risks and hazards of transfusion are in a given community and country, to disseminate these findings and to take appropriate actions including the instigation of appropriate education processes to prevent reccurrence.[20] Similarly haemovigilance data also provide a basis for the wider consideration of product, system and procedural changes that further advance transfusion safety and appropriateness.
The NBA is undertaking the realisation of these objectives through the following initiatives:
Haemovigilance is also supported at a national level by bodies involved in education and practice improvement, production of guidelines, product and service standards and accreditation:
Transfusion-related adverse events are investigated and reported according to local arrangements in each state and territory. A range of staff gather and validate haemovigilance data, including transfusion nurses and other clinical staff, haematologists and other medical specialists, hospital transfusion committees, hospital quality and safety units/managers and pathology quality and safety units/managers.
Serious human errors and incidents are thoroughly investigated at the local level using detailed analytical techniques such as root cause analysis (RCA) to ensure that clinicians and hospital directors fully understand the sequence of events. These procedures already form part of ordinary hospital quality management structures and are also applicable to transfusion practice and transfusion-related adverse events.
Transfusion adverse events are validated locally to properly determine whether they are transfusion-related or not and then imputability scores are allocated. Standards for validation are developed by local institutions in conjunction with health department oversight. Reports of serious adverse events may go through a secondary validation process within the state and territory haemovigilance programs and Department of Health Quality Units to ensure data accuracy and completeness. State and territory haemovigilance representatives, on behalf of health departments, aggregate and de-identify the data and send periodic reports to the NBA. Agreed additional de-identified data concerning the patient, facility, event and implicated blood component will accompany each report, as will an imputability (causality) score, assigned by the reporting jurisdiction.
NSW Health has supported a series of initiatives over the past decade to enhance the quality and safety of transfusion practice in NSW public hospitals. The current transfusion practice improvement program 'Blood Watch' was launched under the auspices of the Clinical Excellence Commission (CEC) in 2006, in collaboration with NSW Health. The primary goal of Blood Watch is to improve the safety and quality of fresh blood component transfusion in all NSW public hospitals through a range of strategies including system redesign, risk controls, education, training and ongoing monitoring and feedback.
All NSW public hospitals use a centralised incident reporting system, the Incident Information Management System (IIMS; based on Adverse Incidents Monitoring System (AIMS), iSOFT Group Ltd) as their only incident reporting tool. IIMS was implemented in all NSW public health facilities in May 2005. The system is designed to allow healthcare professionals to report incidents, including near misses and risks to patient and staff safety. Reporting of incidents and near misses is mandated in the Incident Management Policy Directive PD2007-061.[21]
IIMS includes a specific reporting category for incidents involving blood and blood products which allows the notifier to select the type of blood product involved and the nature of the problem. IIMS also has fields designed to capture a wide range of general incident reporting information, and a free text description of the risk/incident.
Blood/blood product category incidents are included in routine IIMS reports of patterns and trends in reported incidents. In order to derive additional information regarding adverse transfusion events, the CEC performs a targeted analysis of the free text description of adverse events provided within the blood/blood product category of IIMS reports.
All severe adverse events (sentinel events) are subject to RCA investigation. The key lessons derived from the analysis of both severe and less severe events are analysed and strategies to reduce these incidents are developed.
The IIMS system is currently being reviewed. Capacity to report against the ANHDD data items is planned to be incorporated in specifications for its redevelopment.
A key focus in NSW in relation to reducing adverse events associated with transfusion has been to reduce inappropriate transfusion. Since the commencement of the Blood Watch program there has been a 10% reduction in red blood cell transfusions for inpatients in NSW public hospitals. A major focus for the program in 2010 was improving all aspects of identification, treatment and reporting of transfusion-related adverse events.
NSW data is presented in APPENDIX IV.
The STIR system is part of the Blood Matters program.[22] Blood Matters is a collaborative effort between the Department of Health and the Blood Service. Governance of the STIR system is provided by an expert group of clinicians with an interest in adverse event management and transfusion improvement, along with assistance from the Blood Matters secretariat, and it reports to the Blood Matters Advisory Committee (BMAC).
Reporting to STIR is voluntary in VIC. STIR collects haemovigilance data on events from participating public and private hospitals in Victoria and now includes participation from hospitals in TAS, ACT and NT. Victorian public hospitals report clinical incidents into a state-wide reporting system, Victorian Health Incident Management System (VHIMS) which includes blood-related incidents. VHIMS future enhancements will assist with blood incident reporting to align with the STIR criteria, and reduce double reporting for public hospitals in VIC.
Categories of events reportable to STIR are classified as either clinical or procedural.
Clinical:
Procedural:
The electronic system used to manage incident reporting data as part of STIR has been developed within the Blood Matters program. Hospitals submit an initial electronic notification through a web eForm to the STIR office. The STIR office then provides a detailed follow-up investigation form tailored to the type of event notified. This second level reporting by health services collects additional relevant detailed information specific to the event type, and is reported using an electronic Word form. Both initial and second level reports are submitted electronically by email from the reporting health service using the web-based eForm for notification and the investigation. With recent advancements in the STIR system, both forms are imported into the database through a semi-automated process, which has reduced time for the health service and the Blood Matters staff, and provided more timely review and follow up. No information identifying the reporting institution or patient is maintained in the STIR database or visible at review.
In 2009-11, 43 hospitals from VIC, ACT, NT and TAS reported 404 events. Based on information from the Victorian Admitted Episode Dataset, it is estimated for VIC that hospitals which have agreed to report (public and private) represent approximately 85% of the total blood transfusion activity. From 2006-11 clinical incidents events-acute transfusion reactions-comprise 50% of the reports. Procedural events account for approximately 43% of the events, and include incorrect blood component transfused (including transfusion of a unit intended for another patient, or which did not meet a patient's individual requirements, such as failure to provide irradiated components), 'wrong blood in tube' events and other 'near miss' events.
Hospitals are expected to review and validate data prior to submission to STIR. In most institutions this occurs through review by the hospital transfusion committee or senior medical officer. In addition to hospital level validation, the STIR program validates incident data. This includes review, classification and assessment of imputability rating by an expert panel comprised of medical and nursing clinicians and laboratory scientists. If the STIR expert panel rating differs from the hospital's assessment both are recorded, with the STIR rating treated as the primary record. This review is a key strength of the STIR program; it provides validity to the data submitted and recommendations for improved practice. ABO incompatible blood transfusions are also reportable to the Victorian sentinel event program, and an RCA approach for these events is reviewed by the STIR expert group, with comments and recommendations provided back to reporting hospitals through the sentinel event program.
Aggregate information from STIR is presented to BMAC and used to develop policies, recommendations and educational resources for VIC hospitals. STIR reports for 2006-07, 2008-09 and 2009-11 are available at the Blood Matters website http://www.health.vic.gov.au/bloodmatters/tools/stir.htm. Experiences and data from STIR are regularly shared at conferences, workshops and hospital meetings. In the 2009-11 period, 22 formal presentations were given locally (hospital transfusion committees, metropolitan and regional workshops), nationally (Haematology Society of Australia and New Zealand, Australian & New Zealand Society of Blood, Australian Society of Thrombosis and Haemostasis annual scientific meetings and Blood Service Transfusion Update) and internationally (IHN meetings).
Working within established clinical governance structures such as transfusion committees, the availability of transfusion nurses and rural transfusion trainers in Victorian hospitals has been recognised as an important element in supporting developments in transfusion practice improvement, including adverse event reporting, investigation and participation in haemovigilance activities. The emphasis on haemovigilance has been reinforced with the implementation of the NSQHS Standard 7 for hospital accreditation.
Until early 2013, a centralised haemovigilance system was operational across Queensland Health. In this system, data validation and analysis was undertaken by clinicians employed within a corporate division of Queensland Health. The data presented in this report, for 2009-10 and 2010-11, was a product of this centralised haemovigilance system.
After the 2012 restructure of the QLD public health system, Hospital and Health Services (HHSs) were established and are responsible for the quality and safety of clinical services. The continuation of the centralised haemovigilance system was not consistent with the Department of Health's new system manager role and this system ceased in 2013. The QLD haemovigilance system was adapted in line with these new structural arrangements, in which:
HHSs and licensed private health facilities will continue to report incidents and, as required by NSQHS Standard 7, will implement local haemovigilance activities, which may include:
the Department of Health will:
WA Health is implementing patient blood management (PBM) as a standard of care state-wide. The rationale for the introduction of the program includes: the potential to reduce unnecessary patient exposure to the risks associated with avoidable transfusions and the consequent benefits to patients and the blood budget (estimated to be up to five per cent of the WA public healthcare budget); reduced pressure on demand for blood which is expected to increase with the ageing population; a desire to improve informed consent; and growing knowledge of the limitations and potential adverse outcomes with transfusion.
Given the concurrent development of new NSQHS accreditation standards to include transfusion practice, informed transfusion consent and a commitment to improving the appropriateness of transfusion practice, the WA PBM program is an effective strategy to address WA's multiple responsibilities with regard to blood transfusion. The WA PBM program comprises:
WA has finalised the business requirements and tender processes for a new Clinical Incident Monitoring System (CIMS), which is anticipated to include haemovigilance modules. To date, individual hospital-based transfusion committees monitor activities, and investigate transfusion-related incidents in their institutions. The new CIMS will continue to see case review and imputability elements of haemovigilance built into the individual health service programs and where necessary, escalated for a state-wide response.
Haemovigilance data in SA is collected and analysed on an individual hospital or health service basis. The haemovigilance data submission from SA is limited to adverse events reported from across the SA public health system, also known as SA Health. The private sector utilises various incident management systems which are reviewed internally via safety and quality and/or transfusion committees. The Blood Service encourages adverse reaction reporting but primarily receives notification of serious adverse events such as TRALI and suspected bacterial contamination. Product related incidents are predominantly reported through SA Pathology to the Blood Service and may not be captured in hospital-based adverse event systems. SA Health mandates reporting of ABO related haemolytic transfusion reactions through a separate sentinel event reporting process covering public and private hospitals. The reliability of data on reported incidents is dependent on the staff member recognising that a significant adverse event has occurred.
On 1 July 2010, SA Health clinical incident reporting transitioned from AIMS (iSOFT Group Ltd) to Datix Safety Learning System (SLS). SLS is an electronic system for reporting and managing incidents and consumer feedback across the public sector with the capacity for online reporting in addition to reporting via a contact centre. Online reporting has been embraced by hospital staff and the contact centre has since ceased operations. SLS supports:
Designated staff can receive automatic email notifications on transfusion events for their work area when an incident is logged, allowing follow up in real time. Automatic notifications of transfusion events are escalated to management levels within SA Health, depending on the Safety Assessment Code (SAC). BloodSafe Transfusion Nurse Consultants (TNC) are notified of all incidents classified under 'transfusion of blood related problem'. Individual incidents and types of incidents are reviewed and analysed to identify trends and areas of risk.
The ANHDD was taken into consideration during the development of the SLS to facilitate national haemovigilance reporting in addition to meeting general hospital requirements. The quality of the data in SLS should improve, over time, as user knowledge of the software increases and the system evolves as a result of suggested system changes.
Elements of the ANHDD were incorporated into SLS; however, certain fields such as age, sex, date of birth are not mandatory. A single reaction investigation and reporting form has been introduced across SA Health; however, there are no consensus definitions which are aligned with the ANHDD and the form does not capture severity ratings or imputability. SAC scores and free text fields within SLS can aid in the interpretation of events but analysis can be subjective and resource intensive. SA Health does not currently maintain a transfusion specific jurisdictional expert group but significant events will be referred to general hospital or SA Health committees for review.
The system for the investigation, review and management of reported blood and blood component incidents/adverse events in SA is robust due to the collaborative efforts of the SA Department for Health and Ageing, the Blood Service, the SA BloodSafe Program and pathology services. Some reporting gaps remain in terms of both the completeness of individual reports and the overall system coverage across SA Health.
BloodSafe, SA's transfusion practice improvement program, continues to make a significant contribution towards blood transfusion safety and quality improvement. BloodSafe TNC's work in public and private hospitals is aimed at:
SA Health has established a regular reporting and linkage process to monitor fresh blood component utilisation by inpatients. The data linkage will contribute to system understanding of the total volume of components transfused by hospitals.
BloodSafe eLearning Australia is now embedded across SA Health as the main educational tool for hospital staff. It is anticipated that this will result in improvements in the recognition of previously under-reported serious adverse events such as TACO and TRALI.
In TAS, quality and safety activities are undertaken by the blood transfusion team at each major public hospital supported by the Hospital Transfusion Committee (HTC) and local safety and quality governance. TAS is a participant in the Victorian Haemovigilance Program: 'Blood Matters'. This includes reporting to the STIR system, which is administered by the Victorian Department of Health. Tasmanian hospitals are active participants in STIR and have two representatives on the STIR Expert Group.
A state-wide incident reporting system operates across all public sector hospitals and health facilities. The Electronic Incident Management System (EIMS, 'Risk MonitorPro' rL Solutions) is used at local and state-wide levels to report and manage health care incidents as a key component of quality improvement. Department of Health and Human Services is currently scoping a replacement EIMS for the state. Recognising the importance of standardisation of data and related processes, the project team has sought input from the Tasmanian Blood Management Group in the classification design with the key objective of capturing data and supplementing national haemovigilance/NBA reporting in relation to management of safety events.
EIMS currently provides all public hospitals in TAS with a consistent, standard approach to incident reporting. All incidents are followed up and Serious Assessment Code 1 and 2 incidents are referred to a Serious Incident Panel. Blood related incidents represent approximately 1.4% of the total number of incidents reported.
Reporting to STIR is a separate process from EIMS as the two systems are not aligned. A key issue for Tasmania is reporting to a national database. Given that STIR and EIMS are not a good match it appears that provision of information via STIR is the most practical option. It is hoped that the new system will support the extraction of data directly to the STIR system.
Reporting to EIMS is voluntary. However, all Tasmanian public sector hospitals and health facilities use EIMS incident reporting. It is estimated that the private hospitals in TAS represent approximately 10% of the total transfusion activity in the state. All private hospitals record incidents, including blood related incidents, to their own risk management systems, however they do not contribute data to EIMS or STIR. Private hospitals have indicated an interest in contributing towards a state-wide and national database.
Transfusion-related incidents in the public sector are entered into EIMS with follow up incidents according to type and severity. Many haemovigilance activities are coordinated by Blood Transfusion Nurses with positions now in place at each of the four major Tasmanian public hospitals. The role of these positions includes education of clinical staff, development of policies and guidelines, conduct of audits of blood product utilisation and incident reporting and monitoring. Nursing staff undertake the required training in transfusion practice in order to meet the mandatory competency requirements.
There is considerable clinical commitment to haemovigilance in TAS which is reflected in local governance and activities, participation in STIR and involvement in national clinical committees. There are good links with the Blood Service regarding haemovigilance activities. Blood Transfusion Nurses were funded following commencement of the national blood arrangements in order to contribute to jurisdictional requirements of the National Blood Agreement.
Recent initiatives include engagement of rural health facilities with activities undertaken on a regional basis and an ongoing accreditation process in place to designate facilities that have the necessary systems in place to safely transfuse blood. There has also been further engagement with the private hospital sector through education by blood nurses, adoption of forms that are consistent between the public and private sector in each region, and private sector participation on the Blood Transfusion Committee.
Future haemovigilance strategies include:
The ACT is a small jurisdiction with a population of 371,000 people, although the complete catchment covers an extensive area of south-eastern NSW with a total catchment population of over 540,000. The ACT is serviced by two public and four private hospitals that transfuse blood and blood products. These facilities provide transfusion services to their consumers through three pathology providers.
The ACT Health Directorate (the Directorate) is aligned to the Statement on National Stewardship Expectations for the Supply of Blood and Blood Products and adheres to the Statement's Stewardship Principle in regard to collation and management of haemovigilance data. This has been facilitated through the Directorate's cross-jurisdictional collaboration with Blood Matters, VIC. As part of this program the Directorate participates in the STIR system. The ACT's public hospitals use the Riskman general incident reporting system to collect haemovigilance data. The private hospitals currently collect and benchmark their haemovigilance data through their internal organisational quality and risk management systems.
The Canberra Hospital is the region's major public hospital with approximately 600 beds, operating as an acute care tertiary referral centre and a teaching hospital affiliated with the Australian National University.
In addition to adverse event data reporting, the Canberra Hospital regularly participates in clinical transfusion audits conducted by Blood Matters (such as Comparative audit of blood transfusion policy and practice 2011) in addition to local audits and reviews focusing on areas of risk including patient identification, consent, documentation and storage and handling.
ACT data, released for the national haemovigilance report, is validated through a process of review and re-assessment of imputability rating by an expert STIR panel comprised of medical and nursing clinicians and laboratory scientists (including a representative from the ACT). Although the de-identified data is held and reported back to the ACT by STIR, the ACT reports into the National Haemovigilance Program depending on its own assessment.
The ACT being a small jurisdiction has allowed the Directorate's Transfusion Nurse to promote and sustain a jurisdictional approach to haemovigilance in the ACT, aligning transfusion practice across the ACT with national and international guidelines.
The Transfusion Nurse provides clinical leadership in the area of haemovigilance by maintaining a robust system for the investigation, review and management of transfusion-related adverse events, providing education for staff and patients across the ACT, and the development and implementation of clinical policy aligned to national guidelines.
The BloodSafe eLearning Australia program is promoted as critical training for all staff involved in the transfusion chain, at all hospitals across the ACT. Since 2007, the ACT has recorded 3,607 registrations to the program.
Additionally, the Directorate convenes a local blood sector stakeholder group called the Appropriate Use of Blood Reference Group (AUBRG) which has broad-based membership from a variety of stakeholders including the NBA, the Blood Service and clinical representation from each of the hospitals and pathology providers across both the public and private health sectors.
The Directorate has hosted an annual Transfusion Champions Forum since 2009 which has brought together nurses and other health professionals with aims to:
These forums have also been well supported by guest presenters from the NBA, the Blood Service, VIC Blood Matters and the NSW Clinical Excellence Commission.
This forum was the initiating platform for the ACT Transfusion Champions Network.
The aims of this network are:
Future plans for haemovigilance in the ACT include:
The NT Department of Health has established a comprehensive haemovigilance system over the last five years. The system includes:
All NT Network Hospitals use the RiskMan electronic incident management system. All staff members have access to report incidents on RiskMan. Therefore any clinical staff can generate the initial report. Members of the TIRG are alerted by email when a transfusion-related incident is reported on RiskMan. There are four broad transfusion incident categories on RiskMan: administration, transfusion reaction, blood product, and documentation, with each having further sub-categories. The RiskMan system flags any transfusion incidents which meet the STIR criteria. If this occurs, a blood management extension is generated which captures additional information and produces a printable initial STIR report.
A transfusion reaction report is issued with all fresh blood components. If a transfusion reaction occurs, the Transfusion Reaction Report is completed in addition to the RiskMan report. A copy of the Transfusion Reaction Report is sent to the laboratory with any requested specimens. Reporting of transfusion reactions increased 300% with the introduction of the Transfusion Reaction Report in 2010.
The categories of RiskMan incidents which are reportable to STIR, and therefore generate the blood management extension, are:
The TIRG is an expert group which meets monthly to review all transfusion-related incidents occurring in NT Network Hospitals. The group collates and analyses transfusion incident data; ensures serious transfusion incidents are investigated appropriately; coordinates RCA if required; ensures transfusion incidents which meet the STIR criteria are reported to Blood Matters; makes recommendations for transfusion practice improvement; and reports quarterly to the NT Transfusion Committee. The Transfusion Nurse Consultant submits the initial STIR report electronically or by email, and the second level STIR report and investigations are completed by either Transfusion Nurse Consultant or a Hospital Quality Coordinator. The Transfusion Nurse Consultant is the chair of the Transfusion Incident Review Group and provides clinical leadership in haemovigilance across all five NT Network Hospitals.
Since 2010, all five NT Network Hospitals have participated in voluntary reporting to the Blood Matters VIC STIR system. In 2011, a Memorandum of Understanding (MOU) between the VIC Department of Health and the NT Department of Health for the Blood Matters: Better Safer Transfusion Program was finalised. The MOU sets out three schedules covering serious transfusion incident reporting data, clinical audits and bi-annual education forums. All major blood users in VIC, TAS, the ACT and the NT voluntarily report to STIR. Aggregate haemovigilance data is presented in STIR annual reports and is submitted directly to the NBA.
The NTTC, established in 2009, meets quarterly to provide a forum for the review and improvement of blood transfusion services, and to ensure the delivery and use of safe, high quality and cost effective blood.
The NTTC objectives include:
In 2012, the BloodSafe eLearning Australia courses became mandatory for all NT clinical staff involved in the transfusion process. Doctors, nurses and midwives are required to complete the Clinical Transfusion Practice course; phlebotomists are required to complete the Collecting Blood Specimens course; and patient care attendants who transport blood as part of their duties are required to complete the Transporting Blood course. The courses are to be completed on commencement of employment and yearly thereafter. The Clinical Transfusion Practice course includes a module on transfusion reactions.
The Northern Territory has participated in several clinical audits conducted by the ANZSBT and VIC Blood Matters, including ANZSBT Survey of Transfusion Consent Practices 2009, Blood Matters Comparative Audit of Blood Transfusion Policy and Practice 2011 and Blood Matters Audit of Consent for Blood Transfusion 2012. In addition, regular internal audits are conducted to provide data on current transfusion practices and to identify areas of practice which may need improving.
Although blood donation is generally safe, a variety of risks and complications exist, the most common being vasovagal reactions, bruising and citrate-related events. Iron deficiency is a longer term risk of donation. In recent decades, extensive efforts have significantly improved recipient and product safety, but there is still potential to further optimise donor care. Donor vigilance is the systematic monitoring of adverse reactions and incidents in blood donor care with a view to improving quality and safety for blood donors.
Standard international definitions are available for surveillance purposes[i]. A recent comprehensive review[23] on adverse events addresses all types of blood donation including whole blood, plasma, platelet, peripheral blood stem cell, leucocyte and bone marrow donation. It outlines strategies for the prevention and treatment of these events and gives a blueprint for future research in this field.
Donor vigilance in Australia is accomplished by the Blood Service with the exception of those donations not collected by the Blood Service, including peripheral blood stem cell, leucocyte and bone marrow donations. Whilst the Blood Service has collected, analysed and reported on donor vigilance data for many years, national data is included in this report for the first time (see PART 03 DONOR VIGILANCE).
The subject of this report is confined to haemovigilance with respect to fresh blood components, such as red blood cells, platelets, fresh frozen plasma, cryodepleted plasma and cryoprecipitate. The Australian medical community also makes significant use of many plasma and recombinant products.
A range of valuable products is manufactured from plasma through the process of fractionation, in which different proteins found in blood plasma are separated, purified and concentrated into distinct therapeutic products. Most plasma derived products supplied in Australia are manufactured from plasma collected by the Blood Service and fractionated by CSL Behring. Some are imported.
Alternative recombinant product versions of plasma derived products are also available. These are manufactured by the expression of equivalent proteins from genetically engineered cell lines.
Important plasma and recombinant products are:
Health professionals are required to report adverse events that occur as a result of administration of all blood and blood products. It is a requirement under the NSQHS Standard 7[ii] to report all adverse events into that facility's incident management and investigation system, as well as to the state and/or national haemovigilance system. As plasma and recombinant products are classified as medicines, reports of adverse events are directed to the TGA[iii].
The TGA maintains a reporting service for adverse events or defects in medicines in Australia. Information on TGA reporting can be found on the TGA's website[iv] and reports can be submitted in various ways. Each year the TGA receives more than 12,000 reports of suspected adverse events associated with medicines and vaccines. About 40% of these reports come via pharmaceutical companies, and the remainder are reported directly to the TGA by general practitioners (about 15% of all reports), hospitals (20%) and specialists, community pharmacists, state and territory health departments and consumers.
The Australian Bleeding Disorders Registry[v] (ABDR) is a clinical registry for patients in Australia with bleeding disorders. It is administered by the NBA, and used on a daily basis by clinicians in all Australian haemophilia treatment centres to assist in managing the treatment of people with bleeding disorders and to gain a better understanding of the incidence and prevalence of bleeding disorders.
The ABDR includes information on the following types of adverse events (this reporting is additional to the statutory requirement to report to the TGA):
The NBA produces ABDR annual reports and adverse event reporting will become more prominent as the dataset matures.
Intravenous immunoglobulin (IVIg) is a fractionated blood product made from pooled human plasma. It is registered for use in Australia for the treatment of a number of diseases where immunoglobulin replacement or immune modulation therapy is indicated. IVIg is used to treat a growing number of unregistered indications where there is some evidence for its utility. IVIg is a life-saving therapy in appropriately selected patients and clinical circumstances.
Since the 1980s, the demand for IVIg has greatly increased, both internationally and in Australia. In the late 1990s, worldwide shortages prompted action by Australian governments to ensure that IVIg was available for those patients most in need. Since that time, strategies to ensure supply have included:
The continual significant annual growth in IVIg usage, the high cost of IVIg products and the potential for supply shortages have all maintained the focus of Australian governments on ensuring use remains consistent with an evidence-based approach and that IVIg is able to be accessed under the National Blood Arrangements for those patients with the greatest clinical need.
The Criteria for the clinical use of intravenous immunoglobulin[vi] in Australia describes current arrangements for access to IVIg funded under the national blood arrangements and the conditions for its use. The criteria have been developed to help clinicians and medical professionals identify the conditions and circumstances for which the use of IVIg is appropriate and funded.
The TGA collects information from health care professionals on IVIg-related adverse reactions occurring in Australia. The NBA may include data on IVIg-related adverse events in future reports.